

Abstract
【Introduction】Idiopathic Multicentric Castleman's disease (iMCD) is a rare lymphoproliferative disorder without 'standard' treatment. In current study, we aimed to investigate the efficacy and safety of TCP regimen (thalidomide, cyclophosphamide and prednisone) in newly diagnosed iMCD patients.
【Methods】From Jun, 2015 to Jun, 2018, thirty-six newly diagnosed iMCD patients were enrolled. TCP regimen (thalidomide 100mg qn for 1 year and maintained with 100mg qn for the second year; cyclophosphamide 300mg/m2 weekly on d1, 8, 15, 22 out of a 28-day cycle; prednisone 1mg/kg twice a week on d1-2, d8-9, d15-16, d22-23 out of a 28-day cycle) was administrated until death or 'treatment failure'. Data from twenty-five patients whose were followed for at least 24 weeks were extracted and analyzed.
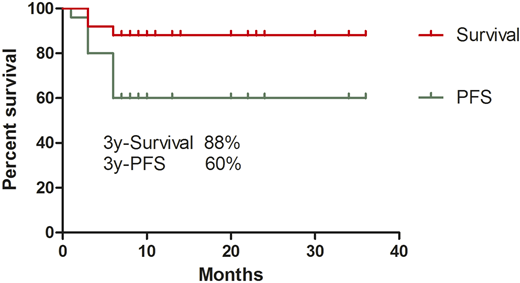
【Results】Among these 25 patients, the median age was 40 years (range 20-63 years), with a male : female ratio of 2.1:1. Two patients fulfilled the diagnostic criteria of TAFRO syndrome. After TCP treatment, 48.0% (n=12) patients achieved 'durable tumor and symptomatic response' for at least 24 weeks; 40.0% (n=10) patients were evaluated as 'treatment failure'; 12.0% (n=3) patients were considered as stable disease. The median symptom score was reduced from 14 (range 6-41) to 3 (range 0-20); the median Interleukin-6 level decreased from 21.3 pg/ml (range 7.4-865) to 9.15pg/ml (range 2.0-36.2). As for safety issues, one patient died from pulmonary infection and one patient suffered from Grade 3 rash. No other patients suffered from Grade 3 or above adverse events. With a median follow-up of 14 months (range 6-36), 8.0% (n=2) patients died: one patient died from progression of disease (severe anemia) and the other died from pulmonary infection after TCP administration. Median overall survival (OS) and progression-free survival (PFS) were not reached, with the estimated 3-year PFS and OS of 60.0% and 88.0%, respectively (Figure 1).
【Conclusions】TCP regimen, an inexpensive oral therapy, is an effective and safe first-line treatment option for newly diagnosed iMCD patients.
No relevant conflicts of interest to declare.

